







A few months ago, I published a post about the Pima Indians (Akimel O'odham) of Arizona. The Pima are one of the most heart-wrenching examples of the disease of civilization afflicting a society after a nutrition transition. Traditionally a healthy agricultural people, they now have some of the highest rates of obesity and diabetes in the world.
The trouble all started when their irrigation waters were diverted upstream in the late 19th century. Their traditional diet of corn, beans, squash, fish, game meats and gathered plant foods became impossible. They became dependent on government food programs, which provided them with white flour, sugar, lard and canned goods. Now they are the subjects of scientific research because of their staggering health problems.
I'm happy to report that after more than 30 years of activism, lawsuits and negotiation, the Pima and neighboring tribes have reached an agreement with the federal government that will restore a portion of their original water. Of the 2 million acre-feet of water the Pima were estimated to have used since before the 16th century, the settlement will restore 653,500. An acre-foot is approximately the personal water use of one household. The settlement also provides federal funds for reconstructing old irrigation canals.
Now we will see how the Pima will use it. Will they return to an agricultural lifestyle, perhaps with the advantages of modern technology? Or will they lease the water rights for money and continue to live off Western foods? Perhaps some of both. They are definitely aware that Western food is causing their health problems, and that they could regain their health by eating traditional foods. However, white flour "fry bread", sugar and canned meat have been around for so long they are also a cultural tradition at this point. Only time will tell which path they choose.
Sunday, August 31, 2008
Yoga
Some cool mini videos from Tara Styles. To view more just click on here profile HERE
Below is one of her videos on strength building with Yoga
This is a preview of the Yoga DVD I use. It's really nice! I love doing yoga to this one!
Also Arturo (another person who does CR) has some good stuff on Yoga here
Below is one of her videos on strength building with Yoga
This is a preview of the Yoga DVD I use. It's really nice! I love doing yoga to this one!
Also Arturo (another person who does CR) has some good stuff on Yoga here
Live to be 150
A good brief introduction into various areas of life extension ideas and research. The program is quite fast paced, but it stays quite interesting all the way through. They cover areas such as life extending drugs such as resveratrol, cryonics, Aubrey De Greys SENS approach to aging, Calorie Restriction, and how others are keeping healthy at an old age.
PART 1
PART 2
PART 3
PART 4
PART 5
PART 6
PART 1
PART 2
PART 3
PART 4
PART 5
PART 6
Saturday, August 30, 2008
Juvess Second Try
It's been a few weeks now since I last tried using Juvess, see belolw to read a bit about the failure! :) Well I have two products now which could help make it work this time
1. Neutrogena Exfoliating gentle face wash to uplug pores and remove dead skin
2. Aloe Vera Gel from Aubrey Organics, which also contains a couple other ingredients like vitamin E and grape seed.
Rather than just using the Juvess all over I'll and apply it to one area like the chin. Which also happens to be where breakouts are more likely to occur because it's in the T zone.
1. Neutrogena Exfoliating gentle face wash to uplug pores and remove dead skin
2. Aloe Vera Gel from Aubrey Organics, which also contains a couple other ingredients like vitamin E and grape seed.
Rather than just using the Juvess all over I'll and apply it to one area like the chin. Which also happens to be where breakouts are more likely to occur because it's in the T zone.
Thursday, August 28, 2008
Conflict of Interest
The U.S. National Cholesterol Education Program (NCEP) is a government organization that educates physicians and the general public about the "dangers" of elevated cholesterol. They have a panel that creates official guidelines for the reduction of cardiovascular disease risk. They contain target cholesterol levels, and the usual recommendations to eat less saturated fat and cholesterol, and lose weight.
They recommend keeping LDL below 100 mg/dL, which would place tens of millions of Americans on statins.
I was reading Dr. John Briffa's blog today and he linked to a government web page disclosing NCEP panel members' conflicts of interest. It's fairly common in academic circles to require conflict of interest statements, so a skeptical audience can decide whether or not they think someone is biased. The 9-member NECP panel was happy to indulge us:
They recommend keeping LDL below 100 mg/dL, which would place tens of millions of Americans on statins.
I was reading Dr. John Briffa's blog today and he linked to a government web page disclosing NCEP panel members' conflicts of interest. It's fairly common in academic circles to require conflict of interest statements, so a skeptical audience can decide whether or not they think someone is biased. The 9-member NECP panel was happy to indulge us:
Every company in bold is a statin manufacturer. This is outrageous! These are the people setting official government blood cholesterol target values for the entire country! Eight out of nine of them should be dismissed immediately, and replaced by people who can do a better job of pretending to be impartial!Dr. Grundy has received honoraria from Merck, Pfizer, Sankyo, Bayer, Merck/Schering-Plough, Kos, Abbott, Bristol-Myers Squibb, and AstraZeneca; he has received research grants from Merck, Abbott, and Glaxo Smith Kline.
Dr. Cleeman has no financial relationships to disclose.
Dr. Bairey Merz has received lecture honoraria from Pfizer, Merck, and Kos; she has served as a consultant for Pfizer, Bayer, and EHC (Merck); she has received unrestricted institutional grants for Continuing Medical Education from Pfizer, Procter & Gamble, Novartis, Wyeth, AstraZeneca, and Bristol-Myers Squibb Medical Imaging; she has received a research grant from Merck; she has stock in Boston Scientific, IVAX, Eli Lilly, Medtronic, Johnson & Johnson, SCIPIE Insurance, ATS Medical, and Biosite.
Dr. Brewer has received honoraria from AstraZeneca, Pfizer, Lipid Sciences, Merck, Merck/Schering-Plough, Fournier, Tularik, Esperion, and Novartis; he has served as a consultant for AstraZeneca, Pfizer, Lipid Sciences, Merck, Merck/Schering-Plough, Fournier, Tularik, Sankyo, and Novartis.
Dr. Clark has received honoraria for educational presentations from Abbott, AstraZeneca, Bristol-Myers Squibb, Merck, and Pfizer; he has received grant/research support from Abbott, AstraZeneca, Bristol-Myers Squibb, Merck, and Pfizer.
Dr. Hunninghake has received honoraria for consulting and speakers bureau from AstraZeneca, Merck, Merck/Schering-Plough, and Pfizer, and for consulting from Kos; he has received research grants from AstraZeneca, Bristol-Myers Squibb, Kos, Merck, Merck/Schering-Plough, Novartis, and Pfizer.
Dr. Pasternak has served as a speaker for Pfizer, Merck, Merck/Schering-Plough, Takeda, Kos, BMS-Sanofi, and Novartis; he has served as a consultant for Merck, Merck/Schering-Plough, Sanofi, Pfizer Health Solutions, Johnson & Johnson-Merck, and AstraZeneca.
Dr. Smith has received institutional research support from Merck; he has stock in Medtronic and Johnson & Johnson.
Dr. Stone has received honoraria for educational lectures from Abbott, AstraZeneca, Bristol-Myers Squibb, Kos, Merck, Merck/Schering-Plough, Novartis, Pfizer, Reliant, and Sankyo; he has served as a consultant for Abbott, Merck, Merck/Schering-Plough, Pfizer, and Reliant.
Wednesday, August 27, 2008
Eating Down the Food Chain
 Europe once teemed with large mammals, including species of elephant, lion, tiger, bear, moose and bison.
Europe once teemed with large mammals, including species of elephant, lion, tiger, bear, moose and bison. America was also home to a number of huge and unusual animals: mammoths, dire wolves, lions, giant sloths and others.
The same goes for Australia, where giant kangaroos, huge wombats and marsupial 'lions' once roamed.
What do these extinctions have in common? They all occurred around when humans arrived. The idea that humans caused them is hotly debated, because they also sometimes coincided with climactic and vegetation changes. However, I believe the fact that these extinctions occurred on several different continents about when humans arrived points to an anthropogenic explanation.
A recent archaeological study from the island of Tasmania off the coast of Australia supports the idea that humans were behind the Australian extinctions. Many large animals went extinct around the time when humans arrived in Australia, but that time also coincided with a change in climate. What the new study shows is that the same large animals survived for another 5,000 years in Tasmania... until humans arrived there from the mainland. Then they promptly went extinct. That time period didn't correspond to a major climate change, so it's hard to explain it away.
It's a harsh reality that our big brains and remarkable adaptability give us the power to be exceptionally destructive to the environment. We're good at finding the most productive niches available, and exploiting them until they implode. Jared Diamond wrote an excellent book on the subject called Collapse, which details how nearly every major civilization collapse throughout history was caused at least in part by environmental damage. It's been a hallmark of human history since the beginning.
I don't think it will take much to convince you that the trend has accelerated in modern times. Ocean life, our major source of nutrient-rich wild food, has already been severely depleted. The current extinction rate is estimated to be over 1,000 times the baseline, pre-modern level, and rising.
Humans have always been top-level predators. We kill and eat nutrient-dense prey that is often much larger than we are. But today, the extinction of such walking meat lockers has caused us to eat down the food chain. We're turning to jellyfish and sea cucumbers and... gasp... lobsters!
While it's true that we've probably always eaten things like shellfish and insects, I find it disturbing that we've depleted the oceans to the point where we can no longer sustainably eat formerly abundant carnivorous fish like tuna. We need to make a concerted effort to preserve these species because extinction is permanent.
I don't want to live in a future where the only thing on the menu is bacteria patties, the other other other other white meat.
Tuesday, August 26, 2008
Cool As A Cucumber Salad with Agave

It started with a visit from a fellow food blogger. And ended up as a side dish. No wait. That doesn't sound right. Because it's more than just a side dish. And the food blogger? Well. She's more than just a food blogger. She's Alanna!
And a certain individual got to make her dinner. Talk about nerve wracking. Cooking for a second-generation food columnist? It's enough to give anyone schpilkis! And I'm no exception. I was afraid I'd burn the quinoa. Or ruin the ribeye. But dinner went off without a hitch. Even with two glasses of wine and a pre-repast stroll to watch the sun set over Abiquiu. I think we talked for five hours.
And the cucumber salad? I made it based on Alanna's simple instructions via cell phone (and via the no-fuss wit and wisdom of Old Liz) and it was such a lip-smacking tasty little number, I ate it for breakfast the next day.
Now that's a good recipe.
Now that's a good recipe.
Thanks Alanna! And muchas gracias to dear Old Liz, who apparently (as we say back east) knows from cucumbers.
Read more + get the recipe >>
Secrets of Living Longer
Secrets of Living Longer
I've spoke about this before but haven't put up this video yet. Dan explains his findings in 3 different areas where there is greater longevity in those that follow certain habits. The most consistent thing is that the poeple who live the longest were mostly vegetarian, they ate little meat and tended to be bean eaters. Seventh Day Adventists for example live upto 10 years longer than the average californian americans and they don't smoke, they don't drink, and they are vegetarian. However they are NOT on CR... as I've previously mentioned their BMI's are around 24 on average (Normal is 18.5-25).
Here are the survival curves for SDA Men and Women

"When vegetarians are forced to take medium-
risk values for all other covariates in the statistical
model, the corresponding expected ages at death are 85.3
and 88.6 years, respectively (Figures 3 and 4)"
Ten Years of Life; Is it a matter of choice?
http://archinte.ama-assn.org/cgi/reprint/161/13/1645
Background: Relative risk estimates suggest that effective
implementation of behaviors commonly advocated
in preventive medicine should increase life expectancy,
although there is little direct evidence.
Objective: To test the hypothesis that choices regarding
diet, exercise, and smoking influence life expectancy.
Methods: A total of 34192 California Seventh-Day Adventists
(75% of those eligible) were enrolled in a cohort
and followed up from 1976 to 1988. A mailed questionnaire
provided dietary and other exposure information
at study baseline. Mortality for all subjects was ascertained
by matching to state death tapes and the National
Death Index.
Results: California Adventists have higher life expectancies
at the age of 30 years than other white Californians
by 7.28 years (95% confidence interval, 6.59-7.97
years) in men and by 4.42 years (95% confidence interval,
3.96-4.88 years) in women, giving them perhaps the
highest life expectancy of any formally described population.
Commonly observed combinations of diet, exercise,
body mass index, past smoking habits, and hormone
replacement therapy (in women) can account for
differences of up to 10 years of life expectancy among
Adventists. A comparison of life expectancy when these
factors take high-risk compared with low-risk values
shows independent effects that vary between 1.06 and
2.74 years for different variables. The effect of each variable
is assessed with all others at either medium- or
high-risk levels.
Conclusions: Choices regarding diet, exercise, cigarette
smoking, body weight, and hormone replacement
therapy, in combination, appear to change life expectancy
by many years. The longevity experience of Adventists
probably demonstrates the beneficial effects of
more optimal behaviors.
I've spoke about this before but haven't put up this video yet. Dan explains his findings in 3 different areas where there is greater longevity in those that follow certain habits. The most consistent thing is that the poeple who live the longest were mostly vegetarian, they ate little meat and tended to be bean eaters. Seventh Day Adventists for example live upto 10 years longer than the average californian americans and they don't smoke, they don't drink, and they are vegetarian. However they are NOT on CR... as I've previously mentioned their BMI's are around 24 on average (Normal is 18.5-25).
Here are the survival curves for SDA Men and Women
"When vegetarians are forced to take medium-
risk values for all other covariates in the statistical
model, the corresponding expected ages at death are 85.3
and 88.6 years, respectively (Figures 3 and 4)"
Ten Years of Life; Is it a matter of choice?
http://archinte.ama-assn.org/cgi/reprint/161/13/1645
Background: Relative risk estimates suggest that effective
implementation of behaviors commonly advocated
in preventive medicine should increase life expectancy,
although there is little direct evidence.
Objective: To test the hypothesis that choices regarding
diet, exercise, and smoking influence life expectancy.
Methods: A total of 34192 California Seventh-Day Adventists
(75% of those eligible) were enrolled in a cohort
and followed up from 1976 to 1988. A mailed questionnaire
provided dietary and other exposure information
at study baseline. Mortality for all subjects was ascertained
by matching to state death tapes and the National
Death Index.
Results: California Adventists have higher life expectancies
at the age of 30 years than other white Californians
by 7.28 years (95% confidence interval, 6.59-7.97
years) in men and by 4.42 years (95% confidence interval,
3.96-4.88 years) in women, giving them perhaps the
highest life expectancy of any formally described population.
Commonly observed combinations of diet, exercise,
body mass index, past smoking habits, and hormone
replacement therapy (in women) can account for
differences of up to 10 years of life expectancy among
Adventists. A comparison of life expectancy when these
factors take high-risk compared with low-risk values
shows independent effects that vary between 1.06 and
2.74 years for different variables. The effect of each variable
is assessed with all others at either medium- or
high-risk levels.
Conclusions: Choices regarding diet, exercise, cigarette
smoking, body weight, and hormone replacement
therapy, in combination, appear to change life expectancy
by many years. The longevity experience of Adventists
probably demonstrates the beneficial effects of
more optimal behaviors.
Saharan Hunter-Gatherers Unearthed
The media recently covered an archaeological discovery in Niger that caught my attention. In the middle of the Sahara desert, researchers found a hunter-gatherer burial site containing over 200 graves ranging from about 10,000 to 4,500 years old. During this period, the region was lush and productive.
There were two groups: the Kiffian, who were powerful hunters and fishermen, and the Tenerian, who were smaller pastoralists (herders) and fishermen.
Individuals at the Kiffian sites averaged over 6 feet tall, with some reaching 6' 8". They were powerfully muscled, and found with the remains of elephants, giraffes, pythons, giant perch and other large game.
Not that you have to be Conan the Barbarian to kill an elephant. Forest pygmies traditionally hunt elephants, and there's a picutre in Nutrition and Physical Degeneration to prove it. They use stealth, agility and an intimate knowledge of their prey to make up for their small size and primitive weapons.
Both the Kiffians and the Tenerians had excellent dental development and health. Take a look at some of the pictures. Those are the teeth of a wild Homo sapiens. Straight, free of decay and with plenty of room for the wisdom teeth. They must have had good dentists.
Both cultures also showed a high level of intelligence and empathy. They were found with decorated pottery shards and their bodies were arranged in imaginative and empathetic ways. A man was buried sitting on a tortoise shell. A mother was buried with her two children. Here's the picture. I can't say it better than the LA Times:
There were two groups: the Kiffian, who were powerful hunters and fishermen, and the Tenerian, who were smaller pastoralists (herders) and fishermen.
Individuals at the Kiffian sites averaged over 6 feet tall, with some reaching 6' 8". They were powerfully muscled, and found with the remains of elephants, giraffes, pythons, giant perch and other large game.
Not that you have to be Conan the Barbarian to kill an elephant. Forest pygmies traditionally hunt elephants, and there's a picutre in Nutrition and Physical Degeneration to prove it. They use stealth, agility and an intimate knowledge of their prey to make up for their small size and primitive weapons.
Both the Kiffians and the Tenerians had excellent dental development and health. Take a look at some of the pictures. Those are the teeth of a wild Homo sapiens. Straight, free of decay and with plenty of room for the wisdom teeth. They must have had good dentists.
Both cultures also showed a high level of intelligence and empathy. They were found with decorated pottery shards and their bodies were arranged in imaginative and empathetic ways. A man was buried sitting on a tortoise shell. A mother was buried with her two children. Here's the picture. I can't say it better than the LA Times:
Among the Tenerian graves was a heart-rending burial tableaux [SIC!!]: A young woman was lying on her side. Pollen under her body suggested that she was placed on a bed of flowers. Lying on their sides facing her were two young children, their fingers interlocked with hers, leaving a tangle of bones.Haha, I couldn't let the spelling error slide, it should be 'tableau'. Hey, I'm half French, give me a break.
Monday, August 25, 2008
Peanut Chicken Stir-Fry
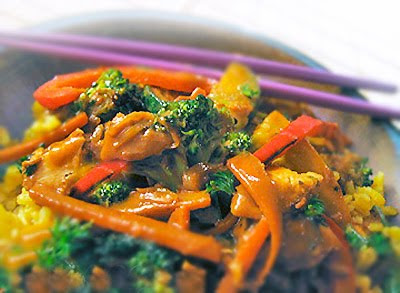
Gluten-free peanut stir-fry sauce- easy to make.
Peanut sauce stir-fry? Yes, please. Spicy peanut sauce is one of my favorite comfort foods. Maybe even in my all-time top ten. The last time I stirred up this peanut sauce we were watching episode 5 of Brideshead Revisited- the most dread inducing episode when it's clear that poor, sweet Sebastian is clinically depressed and Mummy Marchmain (aka the Velvet Hammer) is determined to crush his spirit for propriety's sake. Steve and I were sighing audibly, rooting for dear Sebastian, hoping against hope he would somehow summon the courage to break free from Mummy and stop self medicating as we chop-sticked our way through this lip-smacking bowl of peanutty goodness.
And as we each consumed the last delectable morsels on our licked clean plates we agreed. We just knew this dish would have perked up Sebastian. And Charles, too, for that matter. Nothing like a spicy peanut sauce to fortify you and return some bloom to wan, stoic cheeks.
In need of said fortification but allergic to peanuts, Darling? Don't fret. Substitute Sunbutter in this recipe. Sunflower seed butter has a roasted nut flavor that is delicious in Asian style sauces. [I find it at Whole Foods and Wild Oats.]
So if you're suddenly struck (as I, too often, am) by a craving for peanut stir-fry, imagining tender sweet mouthfuls of crisp broccoli, elegant red pepper strips and slender chicken pieces all commingling happily in an earthy, garlicky peanut sauce, don't worry. I've got you covered. It doesn't get much better than this easy recipe.
Even Sebastian's teddy, Aloysius, could whip this up.
Read more + get the recipe >>
Saturday, August 23, 2008
Fit at 70
In my professional life, I study neurodegenerative disease, the mechanisms of aging, and what the two have in common. I was reading through a textbook on aging a few months ago, and I came across an interesting series of graphs.
The first graph showed the average cardiorespiratory endurance of Americans at different ages. It peaks around 30 and goes downhill from there. But the author of this chapter was very intelligent; he knew that averages sometimes conceal meaningful information. The second graph showed two lines: one representing a man who was sedentary, and the other representing a man who exercised regularly for his entire life. The data were from real individuals. The endurance of the first man basically tracked the national average as he aged. The endurance of the second man remained relatively stable from early adulthood until the age of 70, after which it declined noticeably.
We aren't taking care of ourselves for nothing, ladies and gentlemen. We're doing it because the stakes are high. Just look at Jack LaLanne, the fitness buff. He's been working out regularly and eating a whole foods diet since before I was born, and he's still pumping iron every day at 93.
The first graph showed the average cardiorespiratory endurance of Americans at different ages. It peaks around 30 and goes downhill from there. But the author of this chapter was very intelligent; he knew that averages sometimes conceal meaningful information. The second graph showed two lines: one representing a man who was sedentary, and the other representing a man who exercised regularly for his entire life. The data were from real individuals. The endurance of the first man basically tracked the national average as he aged. The endurance of the second man remained relatively stable from early adulthood until the age of 70, after which it declined noticeably.
We aren't taking care of ourselves for nothing, ladies and gentlemen. We're doing it because the stakes are high. Just look at Jack LaLanne, the fitness buff. He's been working out regularly and eating a whole foods diet since before I was born, and he's still pumping iron every day at 93.
Friday, August 22, 2008
Kitava: Wrapping it Up
There's a lot to be learned from the Kitava study. Kitavans eat a diet of root vegetables, coconut, fruit, vegetables and fish and have undetectable levels of cardiovascular disease (CVD), stroke and overweight. Despite light smoking. 69% of their calories come from carbohydrate, 21% from fat and 10% from protein. This is essentially a carbohydrate-heavy version of what our paleolithic ancestors ate. They also get lots of sunshine and have a moderately high activity level.
The first thing we can say is that a high intake of carbohydrate is not enough, by itself, to cause overweight or the diseases of civilization. It's also not enough to cause insulin resistance. I sent an e-mail to Dr. Lindeberg asking if his group had measured Kitavans' glucose tolerance. He told me they had not. However, I can only guess they had good glucose control since they suffered from none of the complications of unmanaged diabetes.
The Kitavan diet is low in fat, and most of the fat they eat is saturated because it comes from coconuts. Compared to Americans and Swedes, they have a high intake of saturated fat. So much for the theory that saturated fat causes CVD... They also have a relatively high intake of fish fat, at 4g per day. This gives them a high ratio of omega-3 to omega-6 fatty acids, with plenty of DHA and EPA.
Their blood lipid profile is not what a mainstream cardiologist would expect. In fact, it's "worse" than the Swedish profile in many ways, despite the fact that Swedes are highly prone to CVD. This raises the possibility that blood lipids are not causing CVD, but are simply markers of diet and lifestyle factors. That's very easy for me to swallow because it never made sense to me that our livers would try to kill us by secreting triglycerides and withholding HDL. The blood lipid profile that associates best with CVD and metabolic syndrome in the West (but has no relation to them on Kitava) is one that's consistent with a high carbohydrate intake. Where does carbohydrate come from in the West? White flour and sugar maybe?
Kitavans also have very low serum leptin. This may be a keystone to their leanness and health. It suggests that their diet is not interfering with the body's metabolic feedback loops that maintain leanness.
The Kitavan diet is one path to vibrant health. Like many other non-industrial groups, Kitavans eat whole, natural foods that are broadly consistent with what our hunter-gatherer ancestors would have eaten. It amazes me that as humans, we can live well on diets that range from near-complete carnivory to plant-rich omnivory. We are possibly the most adaptable species on the planet.
The ideal diet for humans includes a lot of possibilities. I believe the focus on macronutrients is misguided. There are examples of cultures that were/are healthy eating high-fat diets, high-carbohydrate diets and everything in between. What they do not eat is processed grains, particularly wheat, refined sugar, industrially processed seed oils and other modern foods. I believe these are unhealthy, and this is visible in the trail of destruction they have left around the globe. Its traces can be found in the Pacific islands, where close genetic relatives of the Kitavans have become morbidly obese and unhealthy on a processed-food diet.
The first thing we can say is that a high intake of carbohydrate is not enough, by itself, to cause overweight or the diseases of civilization. It's also not enough to cause insulin resistance. I sent an e-mail to Dr. Lindeberg asking if his group had measured Kitavans' glucose tolerance. He told me they had not. However, I can only guess they had good glucose control since they suffered from none of the complications of unmanaged diabetes.
The Kitavan diet is low in fat, and most of the fat they eat is saturated because it comes from coconuts. Compared to Americans and Swedes, they have a high intake of saturated fat. So much for the theory that saturated fat causes CVD... They also have a relatively high intake of fish fat, at 4g per day. This gives them a high ratio of omega-3 to omega-6 fatty acids, with plenty of DHA and EPA.
Their blood lipid profile is not what a mainstream cardiologist would expect. In fact, it's "worse" than the Swedish profile in many ways, despite the fact that Swedes are highly prone to CVD. This raises the possibility that blood lipids are not causing CVD, but are simply markers of diet and lifestyle factors. That's very easy for me to swallow because it never made sense to me that our livers would try to kill us by secreting triglycerides and withholding HDL. The blood lipid profile that associates best with CVD and metabolic syndrome in the West (but has no relation to them on Kitava) is one that's consistent with a high carbohydrate intake. Where does carbohydrate come from in the West? White flour and sugar maybe?
Kitavans also have very low serum leptin. This may be a keystone to their leanness and health. It suggests that their diet is not interfering with the body's metabolic feedback loops that maintain leanness.
The Kitavan diet is one path to vibrant health. Like many other non-industrial groups, Kitavans eat whole, natural foods that are broadly consistent with what our hunter-gatherer ancestors would have eaten. It amazes me that as humans, we can live well on diets that range from near-complete carnivory to plant-rich omnivory. We are possibly the most adaptable species on the planet.
The ideal diet for humans includes a lot of possibilities. I believe the focus on macronutrients is misguided. There are examples of cultures that were/are healthy eating high-fat diets, high-carbohydrate diets and everything in between. What they do not eat is processed grains, particularly wheat, refined sugar, industrially processed seed oils and other modern foods. I believe these are unhealthy, and this is visible in the trail of destruction they have left around the globe. Its traces can be found in the Pacific islands, where close genetic relatives of the Kitavans have become morbidly obese and unhealthy on a processed-food diet.
Thursday, August 21, 2008
How to prevent infections
Over the years you kind of get to know what helps and what doesn't when it comes to either stopping yourself from becoming sick, or just helping to relieve symptoms and hasten up the process of recovery. So in this post I will focus on what you can do to avoid becoming ill with viral infections. September is coming and when all the kids start going back to school there tends to be an outbreak of colds, and then shortly after the flu, and right now there seems to be a spike in the number of gastroenteritis illness which is mostly likely caused by the norovirus.
Green Tea - Green tea contains a polyphenol compound called epigallocatechin gallate (EGCG). This is usually the most active component against many virses, bacteria and fungi. Green Tea seems to alter the protein around the virus and stop it infecting the cells in the first place [1], but if this fails then green tea actually boosts the immune system. [2].
And another mechanisms from another study [3]
My advice is to replace whatever you drink with green tea. Make sure you get a good quality one however, something like Sencha or Matcha green tea, and from Japan if possible rather than China. The decaf products do comtain less EGCG than the caffeinated also. I believe 3 cups of decaf is equivalent to 1 cup of caffeinated green tea.
Garlic - It has been known for a very long time that garlic was a good anti bacterial, and anti viral. The compound responsible for this is the one that gives off that funny smell when you eat too much... but wouldn't you rather just smell a bit of garlic than be sick? I know I would. There was a report a few years back saying that 'garlic is the common cold cure'. Well not quite, however it does seem to do a remarkable job at reducing the number of colds, and reducing the number of days ill with symptoms. What you do is get 2 cloves of garlic and consume them immediately when you feel a cold coming on, then I eat 2 every 3-4 hours for a couple days... I then just stick to me normal intake of 2-4 per day as a preventative measure. So crush the garlic well and then you could possibly put it on a bit of bread, or if you're really brave try chewing it and swallowing. Be careful you don't burn your mouth because believe me, it is pretty strong and can burn right through the tissue in your mouth easily. From BBC news website that reported on the garlic study
If you actually take a look at the full paper you will see that the people who were taking garlic only had significant symptoms for 1.5 days compared to 5 days in the placebo group!
More studies are definitely needed on garlic and common colds/flu. I have tried it out on a few friends and family members and their colds completely went away within 1 day if caught early enough. It has also worked for me and over the last 14 months since I been trying it I have only felt like I had a cold for about 1/2 a day. The results will vary because it also depends on the hosts immunity to virses as well. Garlic might simply just restore you to normal (average) if you are under stress, sleep deprived, already ill or have some other condition that affects your immunity.
Nasal Irrigation - Sounds disgusting right? Well a recent study was published showing that kids who used products that spray water up the nose such as sterimar help ward of infection. Sterimar contains water and sea salt at the right concentrations similar to that of the human body. Because of the osmotic effect of salt you want to have the right concentration so that it doesn't cause irritation to the nasal lining and even bleeding. But interestingly sea salt (or any salt) actually helps kill bacteria by this method, as well as increasing the action of cilia which is tiny hairs in your nose that remove particles and keep mucous moving. When these stop working or are paralyzed by things like cigarette smoke you can be more susceptible to colds and sinusitis (bacterial infection). You can also buy something called a neti pot which are quite cheap and make up your own using 1/4 of a tea spoon of salt for 500ml water. This seems to work fine for me. Make sure it's cooking salt and not table salt. I personally do not recommend doing this neti wash if you have an active infection because it can easily spread the cold to your ears and block those up, simply because of where the eustachian tubes are located.
Vitamin D3 - Have you been looking at the news lately on this vitamin? It seems like everyday there is positive results coming from studies. A double blind placebo controlled study that was held in new york showed that giving subjects vitamin D3 resulted in 70% less colds and flu. There was another study that took place in a hosptial where a doctor gave his patients over 1000IU of vitamin D3 per day and when there was an outbreak of flu, none of those recieving the vitamin D caught it. I predict that in the UK there will be a big cold and flu season again simply because we've had such a poor summer. The best thing you can possibly do for yourself right now is to make sure that you have high normal level of 1,25(OH)D3. You can order this test from your doctor, but 1000IU capsules should get you within a good range, and 2000IU is almost certainly safe too. If you go down to my previous posts a bit you can view a couple videos on vitamin D that might interest you. Here are some extracts from the medicalnews website.
Steam Inhalation - This is simple but can be quite dangerous so be careful if you decide to do this. Just boil kettle water and put it into a bowl. Then get a towel and put your head under it and breath in the steam. Simple but only seems effective for a short while. I still use the method however.
Ginger - Ginger is a well known anti emetic. Meaning, it prevents sickness and nausea. Some doctors instruct women to use it while pregnant and has morning sickness, other uses are travel sickness, general nausea and indigestion, acid reflux disease. The only one it doesn't seem to be effective for is when use post operatively (after operation with G.A). It can be also used to help unblock the noise and is an weak antiviral so could help with cold symptoms. The best use for this herb is simply when you have a bad stomach and don't like being sick. I have managed not to be sick for almost 6 years because of gingers anti emetic effect.
Red Wine - There was a study on the BBC news website a few years back showing that red wine stops common colds. This is probably due to the resveratrol found in red wine. [5]
Resveratrol also has been succesful at blocking bird flu too. Might be worth keeping this one handy in case of a future outbreak.
Broccoli - Broccoli can restore supressed immune function and also transiently stimulate immune function. The effect is quite dramatic and in-vivo studies show that it stimulates various immune system components to augment the hosts defence against cancer, viruses, bacterial infections and fungi infections.
Diindolylmethane (DIM) Immune Modulating Properties Include:
Stimulation of Interferon-γ Sensitivity by Increasing IFN-γ Receptors
Stimulation of Interferon-γ, G-CSF, IL-6 and IL-12 Production
Synergy with Interferon-γ in Expression of the MHC-I Complex
From DIM activation centre website

I recommend you look at reference [8] and read the results for yourself.
Lactoferrin - Lactoferrin can be found in breast milk, cows milk, whey protein. Your body uses lactoferrin in various places such as saliva, tears, urinary tract to prevent infections. It can also be useful in preventing food poison too. Theres a good article over at LEF that you can take a look at, see HERE
Beta Glucan - The one derived from yeast is best, but oats also have an impact on immune system too. I recommend you view this WIKI article here. Beta Glucan clearly has a massive impact on immunity.
Wash hands How simple is this? Just wash your hands frequently and do it with soap for at least 25 seconds under running water. Do not eat before washing your hands
UTI Infections - This is mostly for the girls as they tend to get these much more than men, but the advice can apply to both. Cranberry juice has severeal mechanisms by which is can stop things like bladder infections. Both because it is acidic and it makes the wall of the bladder slipper so the bacteria can't attach. E coli is most often the culprit in these infections. Another very effective method is to use something called D-Mannose. D mannose is basically a sugar and doesn't get digested, passes into the urine and coats the bladder wall, and the bacteria (only works mostly for E coli) attach to the sugar molecules and flush out... without killing a bacterium too! :D
Dental Infections - There is some evidence that green tea is effective against the bacteria that involved in tooth decay. Abscesses are painful, from experience, and from hearing other peoples cry of pain lol. So apart from your daily routine of brushing, flossing, mouth wash etc... drinking green tea is good for this too!
OK that is all from me today... I hope that some of this information will be of use to you. I hope everyone is able to stay well and free from infection. The above wont always work, but it can help as the evidence shows.
[1] Song JM, Lee KH, Seong BL.
Antiviral effect of catechins in green tea on influenza virus.
Link to study
[2] Rowe CA, Nantz MP, Bukowski JF, Percival SS.
Specific formulation of Camellia sinensis prevents cold and flu symptoms and enhances gamma,delta T cell function: a randomized, double-blind, placebo-controlled study.
Link to study
[3] Garlic 'prevents common cold'
[4] Epidemic Influenza And Vitamin D
[5] Red wine 'protects from colds'
[6] Chemical in grapes inhibits flu virus
[7] Compound in broccoli has immune-boosting properties, finds new study
[8] DIM
Green Tea - Green tea contains a polyphenol compound called epigallocatechin gallate (EGCG). This is usually the most active component against many virses, bacteria and fungi. Green Tea seems to alter the protein around the virus and stop it infecting the cells in the first place [1], but if this fails then green tea actually boosts the immune system. [2].
"Among subjects taking CSF there were 32.1% fewer subjects with symptoms (P = 0.035), 22.9% fewer overall illnesses of at least 2 days duration (P = 0.092), and 35.6% fewer symptom days (P < 0.002), compared to subjects taking placebo. gammadelta T cells from subjects taking CSF proliferated 28% more (P = 0.017) and secreted 26% more IFN-gamma (P = 0.046) in response to gammadelta T cell antigens, as compared to gammadelta T cells from subjects taking placebo. CSF was well-tolerated."
And another mechanisms from another study [3]
The compounds strongly inhibited adsorption of the viruses on red blood cell (RBC). They also restricted the growth of avian influenza virus in ovo with minimum inhibition concentration (MIC) of 5-10 microM far exceeding the neuraminidase (NA) inhibitor oseltamivir or M2 proton channel inhibitor amantadine. The antiviral activity appears to be mediated by interaction with hemagglutinin (HA)/viral membrane rendering HA less fusogenic at the initial stage of infection.
My advice is to replace whatever you drink with green tea. Make sure you get a good quality one however, something like Sencha or Matcha green tea, and from Japan if possible rather than China. The decaf products do comtain less EGCG than the caffeinated also. I believe 3 cups of decaf is equivalent to 1 cup of caffeinated green tea.
Garlic - It has been known for a very long time that garlic was a good anti bacterial, and anti viral. The compound responsible for this is the one that gives off that funny smell when you eat too much... but wouldn't you rather just smell a bit of garlic than be sick? I know I would. There was a report a few years back saying that 'garlic is the common cold cure'. Well not quite, however it does seem to do a remarkable job at reducing the number of colds, and reducing the number of days ill with symptoms. What you do is get 2 cloves of garlic and consume them immediately when you feel a cold coming on, then I eat 2 every 3-4 hours for a couple days... I then just stick to me normal intake of 2-4 per day as a preventative measure. So crush the garlic well and then you could possibly put it on a bit of bread, or if you're really brave try chewing it and swallowing. Be careful you don't burn your mouth because believe me, it is pretty strong and can burn right through the tissue in your mouth easily. From BBC news website that reported on the garlic study
Over a 90-day period during the winter when most colds occur, just 24 colds were recorded among those taking the supplement, compared to 65 amongst those taking the placebo.
The study also found that those taking the supplement who did catch a cold were more likely to make a speedier recovery than those taking the placebo and the chances of re-infection following a cold were significantly reduced
If you actually take a look at the full paper you will see that the people who were taking garlic only had significant symptoms for 1.5 days compared to 5 days in the placebo group!
More studies are definitely needed on garlic and common colds/flu. I have tried it out on a few friends and family members and their colds completely went away within 1 day if caught early enough. It has also worked for me and over the last 14 months since I been trying it I have only felt like I had a cold for about 1/2 a day. The results will vary because it also depends on the hosts immunity to virses as well. Garlic might simply just restore you to normal (average) if you are under stress, sleep deprived, already ill or have some other condition that affects your immunity.
Nasal Irrigation - Sounds disgusting right? Well a recent study was published showing that kids who used products that spray water up the nose such as sterimar help ward of infection. Sterimar contains water and sea salt at the right concentrations similar to that of the human body. Because of the osmotic effect of salt you want to have the right concentration so that it doesn't cause irritation to the nasal lining and even bleeding. But interestingly sea salt (or any salt) actually helps kill bacteria by this method, as well as increasing the action of cilia which is tiny hairs in your nose that remove particles and keep mucous moving. When these stop working or are paralyzed by things like cigarette smoke you can be more susceptible to colds and sinusitis (bacterial infection). You can also buy something called a neti pot which are quite cheap and make up your own using 1/4 of a tea spoon of salt for 500ml water. This seems to work fine for me. Make sure it's cooking salt and not table salt. I personally do not recommend doing this neti wash if you have an active infection because it can easily spread the cold to your ears and block those up, simply because of where the eustachian tubes are located.
Vitamin D3 - Have you been looking at the news lately on this vitamin? It seems like everyday there is positive results coming from studies. A double blind placebo controlled study that was held in new york showed that giving subjects vitamin D3 resulted in 70% less colds and flu. There was another study that took place in a hosptial where a doctor gave his patients over 1000IU of vitamin D3 per day and when there was an outbreak of flu, none of those recieving the vitamin D caught it. I predict that in the UK there will be a big cold and flu season again simply because we've had such a poor summer. The best thing you can possibly do for yourself right now is to make sure that you have high normal level of 1,25(OH)D3. You can order this test from your doctor, but 1000IU capsules should get you within a good range, and 2000IU is almost certainly safe too. If you go down to my previous posts a bit you can view a couple videos on vitamin D that might interest you. Here are some extracts from the medicalnews website.
guess our hospital was under luckier stars as only about 12% of our patients were infected and no one died. However, as the epidemic progressed, I noticed something unusual. First, the ward below mine was infected, and then the ward on my right, left, and across the hall - but no patients on my ward became ill. My patients had intermingled with patients from infected wards before the quarantines. The nurses on my unit cross-covered on infected wards. Surely, my patients were exposed to the influenza A virus. How did my patients escape infection from what some think is the most infectious of all the respiratory viruses?
My patients were no younger, no healthier, and in no obvious way different from patients on other wards. Like other wards, my patients are mostly African Americans who came from the same prisons and jails as patients on the infected wards. They were prescribed a similar assortment of powerful psychotropic medications we use throughout the hospital to reduce the symptoms of psychosis, depression, and violent mood swings and to try to prevent patients from killing themselves or attacking other patients and the nursing staff. If my patients were similar to the patients on all the adjoining wards, why didn't even one of my patients catch the flu?
A short while later, a group of scientists from UCLA published a remarkable paper in the prestigious journal, Nature. The UCLA group confirmed two other recent studies, showing that a naturally occurring steroid hormone - a hormone most of us take for granted - was, in effect, a potent antibiotic. Instead of directly killing bacteria and viruses, the steroid hormone under question increases the body's production of a remarkable class of proteins, called antimicrobial peptides. The 200 known antimicrobial peptides directly and rapidly destroy the cell walls of bacteria, fungi, and viruses, including the influenza virus, and play a key role in keeping the lungs free of infection. The steroid hormone that showed these remarkable antibiotic properties was plain old vitamin D.
Steam Inhalation - This is simple but can be quite dangerous so be careful if you decide to do this. Just boil kettle water and put it into a bowl. Then get a towel and put your head under it and breath in the steam. Simple but only seems effective for a short while. I still use the method however.
Ginger - Ginger is a well known anti emetic. Meaning, it prevents sickness and nausea. Some doctors instruct women to use it while pregnant and has morning sickness, other uses are travel sickness, general nausea and indigestion, acid reflux disease. The only one it doesn't seem to be effective for is when use post operatively (after operation with G.A). It can be also used to help unblock the noise and is an weak antiviral so could help with cold symptoms. The best use for this herb is simply when you have a bad stomach and don't like being sick. I have managed not to be sick for almost 6 years because of gingers anti emetic effect.
Red Wine - There was a study on the BBC news website a few years back showing that red wine stops common colds. This is probably due to the resveratrol found in red wine. [5]
"Rather than directly attacking the flu virus itself, resveratrol seems to block host-cell functions that are essential for viral replication, says the report by Anna T. Palamara and colleagues at the University of Rome. They write that the substance holds promise as a possible weapon against flu."
Resveratrol also has been succesful at blocking bird flu too. Might be worth keeping this one handy in case of a future outbreak.
Broccoli - Broccoli can restore supressed immune function and also transiently stimulate immune function. The effect is quite dramatic and in-vivo studies show that it stimulates various immune system components to augment the hosts defence against cancer, viruses, bacterial infections and fungi infections.
Diindolylmethane (DIM) Immune Modulating Properties Include:
Stimulation of Interferon-γ Sensitivity by Increasing IFN-γ Receptors
Stimulation of Interferon-γ, G-CSF, IL-6 and IL-12 Production
Synergy with Interferon-γ in Expression of the MHC-I Complex
From DIM activation centre website
I recommend you look at reference [8] and read the results for yourself.
Lactoferrin - Lactoferrin can be found in breast milk, cows milk, whey protein. Your body uses lactoferrin in various places such as saliva, tears, urinary tract to prevent infections. It can also be useful in preventing food poison too. Theres a good article over at LEF that you can take a look at, see HERE
Beta Glucan - The one derived from yeast is best, but oats also have an impact on immune system too. I recommend you view this WIKI article here. Beta Glucan clearly has a massive impact on immunity.
Wash hands How simple is this? Just wash your hands frequently and do it with soap for at least 25 seconds under running water. Do not eat before washing your hands
UTI Infections - This is mostly for the girls as they tend to get these much more than men, but the advice can apply to both. Cranberry juice has severeal mechanisms by which is can stop things like bladder infections. Both because it is acidic and it makes the wall of the bladder slipper so the bacteria can't attach. E coli is most often the culprit in these infections. Another very effective method is to use something called D-Mannose. D mannose is basically a sugar and doesn't get digested, passes into the urine and coats the bladder wall, and the bacteria (only works mostly for E coli) attach to the sugar molecules and flush out... without killing a bacterium too! :D
Dental Infections - There is some evidence that green tea is effective against the bacteria that involved in tooth decay. Abscesses are painful, from experience, and from hearing other peoples cry of pain lol. So apart from your daily routine of brushing, flossing, mouth wash etc... drinking green tea is good for this too!
OK that is all from me today... I hope that some of this information will be of use to you. I hope everyone is able to stay well and free from infection. The above wont always work, but it can help as the evidence shows.
[1] Song JM, Lee KH, Seong BL.
Antiviral effect of catechins in green tea on influenza virus.
Link to study
[2] Rowe CA, Nantz MP, Bukowski JF, Percival SS.
Specific formulation of Camellia sinensis prevents cold and flu symptoms and enhances gamma,delta T cell function: a randomized, double-blind, placebo-controlled study.
Link to study
[3] Garlic 'prevents common cold'
[4] Epidemic Influenza And Vitamin D
[5] Red wine 'protects from colds'
[6] Chemical in grapes inhibits flu virus
[7] Compound in broccoli has immune-boosting properties, finds new study
[8] DIM
Cardiovascular Risk Factors on Kitava, Part IV: Leptin
Leptin is a hormone that is a central player in the process of weight gain and chronic disease. Its existence had been predicted for decades, but it was not identified until 1994. Although less well known than insulin, its effects on nutrient disposal, metabolic rate and feeding behaviors place it on the same level of importance.
Caloric intake and expenditure vary from day to day and week to week in humans, yet most people maintain a relatively stable weight without consciously adjusting food intake. For example, I become hungry after a long fast, whereas I won't be very hungry if I've stuffed myself for two meals in a row. This suggests a homeostatic mechanism, or feedback loop, which keeps weight in the body's preferred range. Leptin is the major feedback signal.
Here's how it works. Leptin is secreted by adipose (fat) tissue, and its blood levels are proportional to fat mass. The more fat, the more leptin. It acts in the brain to increase the metabolic rate, decrease eating behaviors, and inhibit the deposition of fat. Thus, if fat mass increases, hunger diminishes and the body tries to burn calories to regain its preferred equilibrium.
The next logical question is "how could anyone become obese if this feedback loop inhibits energy storage in response to fat gain?" The answer is a problem called leptin resistance. In people who are obese, the brain no longer responds to the leptin signal. In fact, the brain believes leptin levels are low, implying stored energy is low, so it thinks it's starving. This explains the low metabolic rate, increased tendency for fat storage and hyperphagia (increased eating) seen in many obese people. Leptin resistance has reset the body's preferred weight 'set-point' to a higher level.
Incidentally, some reaserchers have claimed that obese people gain fat because they don't fidget as much as others. This is based on the observation that thin people fidget more than overweight people. Leptin also influences activity levels, so it's possible that obese people fidget less than thin people due to their leptin resistance. In other words, they fidget less because they're fat, rather than the other way around.
The problem of leptin resistance is well illustrated by a rat model called the Zucker fatty strain. The Zucker rat has a mutation in the leptin receptor gene, making its brain unresponsive to leptin signals. The rat's fat tissue pumps out leptin, but its brain is deaf to it. This is basically a model of severe leptin resistance, the same thing we see in obese humans. What happens to these rats? They become hyperphagic, hypometabolic, obese, develop insulin resistance, impaired glucose tolerance, dyslipidemia, diabetes, and cardiovascular disease. Basically, severe metabolic syndrome.
This shows that leptin resistance is sufficient to cause many of the common metabolic problems that plague modern societies. In humans, it's a little known fact that leptin resistance precedes the development of obesity, insulin resistance, and impaired glucose tolerance! Furthermore, humans with leptin receptor mutations or impaired leptin production become hyperphagic and severely obese. This puts leptin at the top of my list of suspects.
So here we have the Kitavans, who are thin and healthy. How's their leptin? Incredibly low. Even in young individuals, Kitavan leptin levels average less than half of Swedish levels. Beyond age 60, Kitavans have 1/4 the leptin level of Swedish people. The difference is so great, the standard deviations don't even overlap.
This isn't surprising, since leptin levels track with fat mass and the Kitavans are very lean (average male BMI = 20, female BMI = 18). Now we are faced with a chicken and egg question. Are Kitavans thin because they're leptin-sensitive, or are they leptin-sensitive because they're thin?
There's no way to answer this question conclusively using the data I'm familiar with. However, in mice and humans, leptin resistance by itself can initiate a spectrum of metabolic problems very reminiscent of what we see so frequently in modern societies. This leads me to believe that there's something about the modern lifestyle that causes leptin resistance. As usual, my microscope is pointed directly at industrial food.
Caloric intake and expenditure vary from day to day and week to week in humans, yet most people maintain a relatively stable weight without consciously adjusting food intake. For example, I become hungry after a long fast, whereas I won't be very hungry if I've stuffed myself for two meals in a row. This suggests a homeostatic mechanism, or feedback loop, which keeps weight in the body's preferred range. Leptin is the major feedback signal.
Here's how it works. Leptin is secreted by adipose (fat) tissue, and its blood levels are proportional to fat mass. The more fat, the more leptin. It acts in the brain to increase the metabolic rate, decrease eating behaviors, and inhibit the deposition of fat. Thus, if fat mass increases, hunger diminishes and the body tries to burn calories to regain its preferred equilibrium.
The next logical question is "how could anyone become obese if this feedback loop inhibits energy storage in response to fat gain?" The answer is a problem called leptin resistance. In people who are obese, the brain no longer responds to the leptin signal. In fact, the brain believes leptin levels are low, implying stored energy is low, so it thinks it's starving. This explains the low metabolic rate, increased tendency for fat storage and hyperphagia (increased eating) seen in many obese people. Leptin resistance has reset the body's preferred weight 'set-point' to a higher level.
Incidentally, some reaserchers have claimed that obese people gain fat because they don't fidget as much as others. This is based on the observation that thin people fidget more than overweight people. Leptin also influences activity levels, so it's possible that obese people fidget less than thin people due to their leptin resistance. In other words, they fidget less because they're fat, rather than the other way around.
The problem of leptin resistance is well illustrated by a rat model called the Zucker fatty strain. The Zucker rat has a mutation in the leptin receptor gene, making its brain unresponsive to leptin signals. The rat's fat tissue pumps out leptin, but its brain is deaf to it. This is basically a model of severe leptin resistance, the same thing we see in obese humans. What happens to these rats? They become hyperphagic, hypometabolic, obese, develop insulin resistance, impaired glucose tolerance, dyslipidemia, diabetes, and cardiovascular disease. Basically, severe metabolic syndrome.
This shows that leptin resistance is sufficient to cause many of the common metabolic problems that plague modern societies. In humans, it's a little known fact that leptin resistance precedes the development of obesity, insulin resistance, and impaired glucose tolerance! Furthermore, humans with leptin receptor mutations or impaired leptin production become hyperphagic and severely obese. This puts leptin at the top of my list of suspects.
So here we have the Kitavans, who are thin and healthy. How's their leptin? Incredibly low. Even in young individuals, Kitavan leptin levels average less than half of Swedish levels. Beyond age 60, Kitavans have 1/4 the leptin level of Swedish people. The difference is so great, the standard deviations don't even overlap.
This isn't surprising, since leptin levels track with fat mass and the Kitavans are very lean (average male BMI = 20, female BMI = 18). Now we are faced with a chicken and egg question. Are Kitavans thin because they're leptin-sensitive, or are they leptin-sensitive because they're thin?
There's no way to answer this question conclusively using the data I'm familiar with. However, in mice and humans, leptin resistance by itself can initiate a spectrum of metabolic problems very reminiscent of what we see so frequently in modern societies. This leads me to believe that there's something about the modern lifestyle that causes leptin resistance. As usual, my microscope is pointed directly at industrial food.
Wednesday, August 20, 2008
Gluten-Free Pear Polenta Muffins
 |
| Tender and sweet pear polenta muffins. |
Ripe juicy pears and a polenta flour base make this new muffin recipe an instant favorite. I'll mention right off the bat- it's not low carb. It uses a moderate amount of sugar and some rice flour with organic corn meal. But if you're pining for a gluten-free vegan muffin recipe that you will absolutely love and devour with relish and lick your fingers and say softly (in your best Lauren Bacall voice), You know those pear muffins you got over there, Steve? You wanna toss me another?
These are it.
Pear Polenta Muffins Recipe
This recipe is vegan, meaning no eggs or dairy are used. But you'd never know it. These muffins are grainy and tender with soft sweet bites of pear that almost melt in your mouth.
Ingredients:
2 cups peeled, cored and diced ripe pears- 2-3 pears- depending upon size
2 cups peeled, cored and diced ripe pears- 2-3 pears- depending upon size
3/4 cup gluten-free cornmeal
3/4 cup brown rice flour or sorghum flour
or sorghum flour
1/4 cup tapioca starch
1 teaspoon sea salt
1 tablespoon baking powder
1 teaspoon ground cinnamon
1/4 cup light olive oil
1 soft ripe banana, mashed well
1/3 to 1/2 cup hemp or rice milk, as needed
2/3 cup organic brown or raw sugar
1 tablespoon bourbon vanilla extract
A sprinkle of organic raw sugar for topping, if desired
for topping, if desired
Instructions:
Preheat the oven to 350ºF. Line a twelve muffin tin with liners.
with liners.
Preheat the oven to 350ºF. Line a twelve muffin tin
In a large bowl combine the dry ingredients- cornmeal, rice flour, tapioca starch, sea salt, baking powder and cinnamon; whisk with a fork to blend. Set aside.
In a separate bowl beat the light olive oil with the mashed banana; add 1/3 cup hemp milk, sugar and vanilla; beat until smooth.
Add the wet mixture into the dry ingredients and beat lightly until well blended; but do not beat it to death. The batter should be like a thick muffin batter (not as thin as a cake batter). If your batter is dry or stiff add a tablespoon of hemp or rice milk at a time and stir until it loosens up.
Stir in the pears.
Drop the batter into the muffin cups by spoonfuls; distribute evenly among the twelve cups. I like to make sure there are a few pear pieces sticking out of the tops. Sprinkle with a dusting of raw sugar.
Bake in the center of a preheated oven for 20 to 25 minutes or so until the muffins are firm to the touch on top and a wooden pick inserted into the center emerges clean. Try the pick method twice- you might hit a moist pear.
Set the pan on a rack to cool for a couple of minutes; then liberate the muffins from the hot pan- this keeps the bottoms from steaming and getting soggy. Cool the muffins on a wire rack.


To store- wrap and freeze cooled muffins in the freezer. They thaw easily and taste tender and sweet when still a wee bit chilled. They also are delicious warm.
Makes 12 muffins.
Tip: Room temperature pears help keep the baking time even; room temperature ingredients work best in gluten-free baking.
Recipe Source: glutenfreegoddess.blogspot.com
All images & content are copyright protected, all rights reserved. Please do not use our images or content without prior permission. Thank you.

Monday, August 18, 2008
Cardiovascular Risk Factors on Kitava, Part III: Insulin
The Kitava study continues to get more and more interesting in later publications. Dr. Lindeberg and his colleagues continued exploring disease markers in the Kitavans, perhaps because their blood lipid findings were not consistent with what one would expect to find in a modern Western population with a low prevalence of CVD.
In their next study, the researchers examined Kitavans' insulin levels compared to Swedish controls. This paper is short but very sweet. Young Kitavan men and women have a fasting serum insulin level considerably lower than their Swedish counterparts (KM 3.9 IU/mL; SM 5.7; KW 3.5; SW 6.2). Kitavan insulin is relatively stable with age, whereas Swedish insulin increases. In the 60-74 year old group, Kitavans have approximately half the fasting serum insulin of Swedes. One thing to keep in mind is that these are average numbers. There is some overlap between the Kitavan and Swedish numbers, with a few Kitavans above the Swedish mean.
In figure 2, they address the possibility that exercise is the reason for Kitavans' low insulin levels. Kitavans have an activity level comparable to a moderately active Swedish person. They divided the Swedes into three categories: low, medium, and high amounts of physical activity at work. The people in the "low" category had the highest insulin, followed by the "high" group and then the "medium" group. The differences were small, however, and Kitavans had far lower serum insulin, on average, than any of the three Swedish groups. These data show that exercise can not explain Kitavans' low insulin levels.
The researchers also found that they could accurately predict average Swedish and Kitavan insulin levels using an equation that factored in age, BMI and waist circumference. This shows that there is a strong correlation between body composition and insulin levels, which applies across cultures.
Now it's time to take a step back and do some interpreting. First of all, this paper is consistent with the idea (but does not prove) that elevated insulin is a central element of overweight, vascular disease and possibly the other diseases of civilization. While we saw previously that mainstream blood lipid markers do not correlate well with CVD or stroke on Kitava, insulin has withstood the cross-cultural test.
In my opinion, the most important finding in this paper is that a high-carbohydrate diet does not necessarily lead to elevated fasting insulin. This is why I think the statement "carbohydrate drives insulin drives fat" is an oversimplification. With a properly-functioning pancreas and insulin-sensitive tissues (which many people in industrial societies do not have), a healthy person can eat a high-carbohydrate meal and keep blood glucose under control. Insulin definitely spikes, but it's temporary. The rest of the day, insulin is at basal levels. The Kitavans show that insulin spikes per se do not cause hyperinsulinemia.
So this leads to the Big Question: what causes hyperinsulinemia?? The best I can give you is informed speculation. Who has hyperinsulinemia? Industrial populations, especially the U.S. and native populations that have adopted Western foods. Who doesn't? Non-industrial populations that have not been affected by Western food habits, including the traditional Inuit, the Kuna, the traditional Masai and the Kitavans.
We can guess that total fat, saturated fat and carbohydrate do not cause hyperinsulinemia, based on data from the Inuit, the Masai and the Kitavans, respectively. We can also guess that there's not some specific food that protects these populations, since they eat completely different things. Exercise also can not completely account for these findings. What does that leave us with? Western food habits. In my opinion, the trail of metabolic destruction that has followed Westerners throughout the world is probably due in large part to industrial foods, including refined wheat flour, sugar and seed oils.
I'm not the first person to come up with this idea, far from it. The idea that specific types of carbohydrate foods, rather than carbohydrate in general, are responsible for the diseases of civilization, has been around for at least a century. It was an inescapable conclusion in the time of Weston Price, when anthropologists and field physicians could observe the transitions of native people to Western diets all over the world. This information has gradually faded from our collective consciousness as native cultures have become increasingly rare. The Kitava study is a helpful modern-day reminder.
In their next study, the researchers examined Kitavans' insulin levels compared to Swedish controls. This paper is short but very sweet. Young Kitavan men and women have a fasting serum insulin level considerably lower than their Swedish counterparts (KM 3.9 IU/mL; SM 5.7; KW 3.5; SW 6.2). Kitavan insulin is relatively stable with age, whereas Swedish insulin increases. In the 60-74 year old group, Kitavans have approximately half the fasting serum insulin of Swedes. One thing to keep in mind is that these are average numbers. There is some overlap between the Kitavan and Swedish numbers, with a few Kitavans above the Swedish mean.
In figure 2, they address the possibility that exercise is the reason for Kitavans' low insulin levels. Kitavans have an activity level comparable to a moderately active Swedish person. They divided the Swedes into three categories: low, medium, and high amounts of physical activity at work. The people in the "low" category had the highest insulin, followed by the "high" group and then the "medium" group. The differences were small, however, and Kitavans had far lower serum insulin, on average, than any of the three Swedish groups. These data show that exercise can not explain Kitavans' low insulin levels.
The researchers also found that they could accurately predict average Swedish and Kitavan insulin levels using an equation that factored in age, BMI and waist circumference. This shows that there is a strong correlation between body composition and insulin levels, which applies across cultures.
Now it's time to take a step back and do some interpreting. First of all, this paper is consistent with the idea (but does not prove) that elevated insulin is a central element of overweight, vascular disease and possibly the other diseases of civilization. While we saw previously that mainstream blood lipid markers do not correlate well with CVD or stroke on Kitava, insulin has withstood the cross-cultural test.
In my opinion, the most important finding in this paper is that a high-carbohydrate diet does not necessarily lead to elevated fasting insulin. This is why I think the statement "carbohydrate drives insulin drives fat" is an oversimplification. With a properly-functioning pancreas and insulin-sensitive tissues (which many people in industrial societies do not have), a healthy person can eat a high-carbohydrate meal and keep blood glucose under control. Insulin definitely spikes, but it's temporary. The rest of the day, insulin is at basal levels. The Kitavans show that insulin spikes per se do not cause hyperinsulinemia.
So this leads to the Big Question: what causes hyperinsulinemia?? The best I can give you is informed speculation. Who has hyperinsulinemia? Industrial populations, especially the U.S. and native populations that have adopted Western foods. Who doesn't? Non-industrial populations that have not been affected by Western food habits, including the traditional Inuit, the Kuna, the traditional Masai and the Kitavans.
We can guess that total fat, saturated fat and carbohydrate do not cause hyperinsulinemia, based on data from the Inuit, the Masai and the Kitavans, respectively. We can also guess that there's not some specific food that protects these populations, since they eat completely different things. Exercise also can not completely account for these findings. What does that leave us with? Western food habits. In my opinion, the trail of metabolic destruction that has followed Westerners throughout the world is probably due in large part to industrial foods, including refined wheat flour, sugar and seed oils.
I'm not the first person to come up with this idea, far from it. The idea that specific types of carbohydrate foods, rather than carbohydrate in general, are responsible for the diseases of civilization, has been around for at least a century. It was an inescapable conclusion in the time of Weston Price, when anthropologists and field physicians could observe the transitions of native people to Western diets all over the world. This information has gradually faded from our collective consciousness as native cultures have become increasingly rare. The Kitava study is a helpful modern-day reminder.
Free 5 day pass
I just spoke to David Lloyd Health club yesterday because my friend recommended me for a free 5 day pass (or was it 3? will have to ask my friend again). I really want to start building up my strength as I said in my previous post. Last time I managed to bench about 70kg weights, which is actually not bad at all for weighing something around 50kg. I'll probably start slow because I'd rather not risk any injuries... . I think I'm probably going to gain a few pounds of muscle and see how I feel then. Mostly I'm dong this for bone health though because with CR that is of course very important. We don't want fractures so starting weight bearing exercises at a young age is a good idea :)
Nothing really new in terms of any changes to my CR lately, and I'll probably be doing a repeat of a few blood tests as the last ones had a few unexpected numbers. I'm sure everything will be fine now, things are looking up :D
Hope everyone is dong well, and CR is going good...
Nothing really new in terms of any changes to my CR lately, and I'll probably be doing a repeat of a few blood tests as the last ones had a few unexpected numbers. I'm sure everything will be fine now, things are looking up :D
Hope everyone is dong well, and CR is going good...
Sunday, August 17, 2008
Italian-Paleo Eggplant with Crumbled Beef, Tomatoes and Mint
 |
| Gluten-free eggplant recipe with crumbled beef, tomatoes and mint. |
Mediterranean Flavors
The classic Italian flavors are all here- eggplant, tomato, garlic, onion and oregano with a twist of fresh chopped mint nudging it over into Greek territory- but there's not a speck of gluten or dairy.
Mediterranean goodness on a plate.
This recipe is for those of us who miss eggplant Parmesan- a little something I threw together this week when my craving for a slab of eggplant Parm (as we called it back in Massachusetts) heated up to such a fever pitch that all I could think about was, How? How to translate a dish so fiercely reliant on a fried breadcrumb coating and slabs of melty Parmesan cheese? A dish so not gluten-free. Or dairy-free. Or lower glycemic friendly to this waist-whittling goddess.
Thin, weeped eggplant slices are brushed lightly with a little extra virgin olive oil and roasted in a hot oven- all by their lonesome. This makes for a delicate, slightly crispy eggplant slice, let me tell you. Topped with a homemade ragu of Italian tomatoes, browned ground organic beef with onions and garlic and herbs and a splash of balsamic vinegar- it's love, Mediterranean style. It is sustenance. It is flavor. And it's dairy-free.
Saturday, August 16, 2008
Cardiovascular Risk Factors on Kitava, Part II: Blood Lipids
The findings in the previous post are all pretty much expected in a population that doesn't get heart disease. However, things started to get interesting when Lindeberg's group measured the Kitavans' serum lipids ("cholesterol"). Kitavan and Swedish total cholesterol is about the same in young men, around 174 mg/dL (4.5 mmol/L). It rises with age in older Swedish men but not Kitavans.
Doctors commonly refer to total cholesterol over 200 mg/dL (5.2 mmol/L) as "high", so Kitavan men are in the clear. On the other hand, Kitavan women should be dying of heart disease left and right with their high middle-age cholesterol of 247 mg/dL (6.4 mmol/L)! That's actually higher than the value for Swedish women of the same age, who are far more prone to heart disease than Kitavans.
The fun doesn't stop there. Total cholesterol isn't a good predictor of heart attack risk, but there are better measures. LDL on Kitava is lower in males than in Sweden, but for females it's about the same until old age. HDL is slightly lower than Swedes' at middle and old age, and triglycerides are higher on average. Judging by these numbers, Kitavans should have cardiovascular disease (CVD) comparable to Swedes, who suffer from a high rate of cardiovascular mortality.
Kitavan smokers had a lower HDL than nonsmokers, yet still did not develop CVD. Smoking is considered one of the most powerful risk factors for cardiovascular disease in Western populations. I think it's worth noting, however, that Kitavans tend to be light smokers.
These data are difficult to reconcile with the hypothesis that certain patterns of blood lipids cause CVD. Kitavans, particularly the women, have a blood lipid profile that should have them clutching their chests, yet they remain healthy.
There is a theory of the relationship between blood lipids and CVD that can explain these data. Perhaps blood lipids, rather than causing CVD, simply reflect diet composition and other lifestyle factors. Both on Kitava and in the West, low HDL and elevated triglycerides imply a high carbohydrate intake. Low-carbohydrate diets consistently raise HDL and lower triglycerides. On Kitava, carbohydrate comes mostly from root crops. In the West, it comes mostly from processed grains (typically wheat) and sugar. So the blood lipid pattern that associates best with CVD and the metabolic syndrome in the West is simply a marker of industrial food intake.
Doctors commonly refer to total cholesterol over 200 mg/dL (5.2 mmol/L) as "high", so Kitavan men are in the clear. On the other hand, Kitavan women should be dying of heart disease left and right with their high middle-age cholesterol of 247 mg/dL (6.4 mmol/L)! That's actually higher than the value for Swedish women of the same age, who are far more prone to heart disease than Kitavans.
The fun doesn't stop there. Total cholesterol isn't a good predictor of heart attack risk, but there are better measures. LDL on Kitava is lower in males than in Sweden, but for females it's about the same until old age. HDL is slightly lower than Swedes' at middle and old age, and triglycerides are higher on average. Judging by these numbers, Kitavans should have cardiovascular disease (CVD) comparable to Swedes, who suffer from a high rate of cardiovascular mortality.
Kitavan smokers had a lower HDL than nonsmokers, yet still did not develop CVD. Smoking is considered one of the most powerful risk factors for cardiovascular disease in Western populations. I think it's worth noting, however, that Kitavans tend to be light smokers.
These data are difficult to reconcile with the hypothesis that certain patterns of blood lipids cause CVD. Kitavans, particularly the women, have a blood lipid profile that should have them clutching their chests, yet they remain healthy.
There is a theory of the relationship between blood lipids and CVD that can explain these data. Perhaps blood lipids, rather than causing CVD, simply reflect diet composition and other lifestyle factors. Both on Kitava and in the West, low HDL and elevated triglycerides imply a high carbohydrate intake. Low-carbohydrate diets consistently raise HDL and lower triglycerides. On Kitava, carbohydrate comes mostly from root crops. In the West, it comes mostly from processed grains (typically wheat) and sugar. So the blood lipid pattern that associates best with CVD and the metabolic syndrome in the West is simply a marker of industrial food intake.
Friday, August 15, 2008
Cardiovascular Risk Factors on Kitava, Part I: Weight and Blood Pressure
The Kitavans are an isolated population free of cardiovascular disease and stroke, despite the fact that more than three quarters of them smoke cigarettes (although not very frequently). They eat a carbohydrate-heavy, whole-foods diet that is uninfluenced by modern food habits and consists mostly of starchy root crops, fruit, vegetables, coconut and fish. Their intake of grains and processed foods is negligible.
Naturally, when Dr. Lindeberg's group discovered that Kitavans don't suffer from heart disease or stroke, they investigated further. In the second paper of the series, they analyzed the Kitavans' "cardiovascular risk factors" that sometimes associate with heart disease in Western populations, such as overweight, hypertension, elevated total cholesterol and other blood lipid markers.
Kitavans are lean. Adult male body mass index (BMI) starts out at 22, and diminishes with age. For comparison, Swedes begin at a BMI of 25 and stay that way. Both populations lose muscle mass with age, so Kitavans are staying lean while Swedes are gaining fat. The average American has a BMI of about 28, which is considered overweight and 2 points away from being obese.
Kitavans also have a low blood pressure that rises modestly with age. This is actually a bit surprising to me, since other non-industrial groups like the Kuna do not experience a rise in blood pressure with age. Compared with Swedes, Kitavans' blood pressure is considerably lower at all ages.
In the next post, I'll discuss the Kitavans' blood lipid numbers ("cholesterol"), which challenge current thinking about heart disease risk factors.
Naturally, when Dr. Lindeberg's group discovered that Kitavans don't suffer from heart disease or stroke, they investigated further. In the second paper of the series, they analyzed the Kitavans' "cardiovascular risk factors" that sometimes associate with heart disease in Western populations, such as overweight, hypertension, elevated total cholesterol and other blood lipid markers.
Kitavans are lean. Adult male body mass index (BMI) starts out at 22, and diminishes with age. For comparison, Swedes begin at a BMI of 25 and stay that way. Both populations lose muscle mass with age, so Kitavans are staying lean while Swedes are gaining fat. The average American has a BMI of about 28, which is considered overweight and 2 points away from being obese.
Kitavans also have a low blood pressure that rises modestly with age. This is actually a bit surprising to me, since other non-industrial groups like the Kuna do not experience a rise in blood pressure with age. Compared with Swedes, Kitavans' blood pressure is considerably lower at all ages.
In the next post, I'll discuss the Kitavans' blood lipid numbers ("cholesterol"), which challenge current thinking about heart disease risk factors.
Ready to go back, almost
I'm almost ready to get back into karate! My Yoga is going quite good at the moment and doing it twice a week. Now that I recovered about 95% from that cipro poison I need to start building back to how I was before that stuff happened.
One thing has changed however, my mind is saying to be 'gain weight'. I dont particularly like looking skinny as I do, in fact I think I would look healthier by gaining at least 5-10 lbs more. The thing is, if I want to stay true to my beliefs and use the only method known right now to slow ageing, then by sticking with CR I 'could' make it to 'escape velocity' and Aubrey De Grey puts it. But you know, given my age which is only 23, 24 soon (noooo!), I would probably make it anyway without moderate CR... if you believe in the Kurzweil future lol.
There is one thing I'd never go back to though, and that is eating a shitty diet. Vegetables, fruits, nuts, legumes, not forgetting the bit of dark chocolate lol, and I'm pretty happy. It tastes far better than any junk food out there :D
One thing has changed however, my mind is saying to be 'gain weight'. I dont particularly like looking skinny as I do, in fact I think I would look healthier by gaining at least 5-10 lbs more. The thing is, if I want to stay true to my beliefs and use the only method known right now to slow ageing, then by sticking with CR I 'could' make it to 'escape velocity' and Aubrey De Grey puts it. But you know, given my age which is only 23, 24 soon (noooo!), I would probably make it anyway without moderate CR... if you believe in the Kurzweil future lol.
There is one thing I'd never go back to though, and that is eating a shitty diet. Vegetables, fruits, nuts, legumes, not forgetting the bit of dark chocolate lol, and I'm pretty happy. It tastes far better than any junk food out there :D
Two different paths
I got asked a question today about what I'm going to do when I go to university. As medicine has been my goal now for quite a while I just said that, and forgot about the amount of thought I put into deciding over the last few months. It's true that I'd be happy with biomedical science, but medicine is my ideal job, I think. I have to decide really quickly what to do because by the time I'd finish I'd be over 30 years of age... well, maybe not so bad considering CR will keep me younger for longer... but those that have been reading my blog now know by now that I do want to get involved in researching into ageing too. Medical school would be like 6 years, thats including foundation year, and a degree in something like biomedical science would be half that. There is no saying that I'll even make my first attempt to get into med school, but it sure is a decision that I would want to make sure I'm doing the right thing -- the stress of long hours would age me lol.
There is always another idea and that is to go into med school as a grad student, complete biomedical degree and then apply for 4 year course in medicine. I really do have some big decisions to make, and pretty soon, if I am to apply for 2009... Biomedical science I have a bit more time to decide as you don't have to apply so early for that.
But I wont think no more about this now, it's 5am as I type this and I have work at 1pm... I am going to be tiiirrreeed today! :(
There is always another idea and that is to go into med school as a grad student, complete biomedical degree and then apply for 4 year course in medicine. I really do have some big decisions to make, and pretty soon, if I am to apply for 2009... Biomedical science I have a bit more time to decide as you don't have to apply so early for that.
But I wont think no more about this now, it's 5am as I type this and I have work at 1pm... I am going to be tiiirrreeed today! :(
Thursday, August 14, 2008
South Beach Diet Notes- Phase 1

Summer fresh organic yellow tomatoes topped with mint, thyme and scallions, then drizzled with extra virgin olive oil and balsamic vinegar. What more could you ask for? A low glycemic snack with my favorite Mediterranean flavors. And no b-word.
I'm deep into my first week on the South Beach Diet, whittling down my waist a half pound at a time. I am seeing a difference already. And what's really interesting- for this gluten-free pasta and muffin loving girl? After eating a lower glycemic index recipe I don't feel stuffed. Or heavy. Or that other word. The b-word. The word every celiac hates more than anything. Yup. You women out there know what I'm talking about it.
Bloated.
The Kitavans: Wisdom from the Pacific Islands
There are very few cultures left on this planet that have not been affected by modern food habits. There are even fewer that have been studied thoroughly. The island of Kitava in Papua New Guinea is host to one such culture, and its inhabitants have many profound things to teach us about diet and health.
The Kitava study, a series of papers produced primarily by Dr. Staffan Lindeberg and his collaborators, offers a glimpse into the nutrition and health of an ancient society, using modern scientific methods. This study is one of the most complete and useful characterizations of the diet and health of a non-industrial society I have come across. It's also the study that created, and ultimately resolved, my cognitive dissonance over the health effects of carbohydrate.
From the photos I've seen, the Kitavans are beautiful people. They have the broad, attractive faces, smooth skin and excellent teeth typical of healthy non-industrial peoples.
Like the Kuna, Kitavans straddle the line between agricultural and hunter-gatherer lifestyles. They eat a diet primarily composed of tubers (yam, sweet potato, taro and cassava), fruit, vegetables, coconut and fish, in order of calories. This is typical of traditional Pacific island cultures, although the relative amounts differ.
Grains, refined sugar, vegetable oils and other processed foods are virtually nonexistent on Kitava. They get an estimated 69% of their calories from carbohydrate, 21% from fat, 17% from saturated fat and 10% from protein. Most of their fat intake is saturated because it comes from coconuts. They have an omega-6 : omega-3 ratio of approximately 1:2. Average caloric intake is 2,200 calories per day (9,200 kJ). By Western standards, their diet is high in carbohydrate, high in saturated fat, low in total fat, a bit low in protein and high in calories.
Now for a few relevant facts before we really start diving in:
Overall, Kitavans possess a resistance to degenerative diseases that is baffling to industrialized societies. Not only is this typical of non-industrial cultures, I believe it represents the natural state of existence for Homo sapiens. Like all other animals, humans are healthy and robust when occupying their preferred ecological niche. Our niche happens to be a particularly broad one, ranging from near-complete carnivory to plant-rich omnivory. But it does not include large amounts of industrial foods.
In the next few posts, I'll discuss more specific data about the health of the Kitavans.
The Kitava study, a series of papers produced primarily by Dr. Staffan Lindeberg and his collaborators, offers a glimpse into the nutrition and health of an ancient society, using modern scientific methods. This study is one of the most complete and useful characterizations of the diet and health of a non-industrial society I have come across. It's also the study that created, and ultimately resolved, my cognitive dissonance over the health effects of carbohydrate.
From the photos I've seen, the Kitavans are beautiful people. They have the broad, attractive faces, smooth skin and excellent teeth typical of healthy non-industrial peoples.
Like the Kuna, Kitavans straddle the line between agricultural and hunter-gatherer lifestyles. They eat a diet primarily composed of tubers (yam, sweet potato, taro and cassava), fruit, vegetables, coconut and fish, in order of calories. This is typical of traditional Pacific island cultures, although the relative amounts differ.
Grains, refined sugar, vegetable oils and other processed foods are virtually nonexistent on Kitava. They get an estimated 69% of their calories from carbohydrate, 21% from fat, 17% from saturated fat and 10% from protein. Most of their fat intake is saturated because it comes from coconuts. They have an omega-6 : omega-3 ratio of approximately 1:2. Average caloric intake is 2,200 calories per day (9,200 kJ). By Western standards, their diet is high in carbohydrate, high in saturated fat, low in total fat, a bit low in protein and high in calories.
Now for a few relevant facts before we really start diving in:
- Kitavans are moderately active. They have an activity level comparable to a moderately active Swede, the population to which Dr. Lindeberg draws frequent comparisons.
- They have abundant food, and shortage is uncommon.
- Their good health is probably not related to genetics, since genetically similar groups in the same region are exquisitely sensitive to the ravages of industrial food. Furthermore, the only Kitavan who moved away from the island to live a modern life is also the only fat Kitavan.
- Their life expectancy at birth is estimated at 45 years (includes infant mortality), and life expectancy at age 50 is an additional 25 years. This is remarkable for a culture with limited access to modern medicine.
- Over 75% of Kitavans smoke cigarettes, although in small amounts. Even the most isolated societies have their modern vices.
For the whole of PNG, no case of IHD or atherothrombotic stroke has been reported in clinical investigations and autopsy studies among traditionally living Melanesians for more than seven decades, though an increasing number of myocardial infarctions [heart attacks] and angina pectoris in urbanized populations have been reported since the 1960s.Dementia was not found except in in two young Kitavans, who were born handicapped. The elderly remained sharp until death, including one man who reached 100 years of age. Kitavans are also unfamiliar with external cancers, with the exception of one possible case of breast cancer in an elderly woman.
Overall, Kitavans possess a resistance to degenerative diseases that is baffling to industrialized societies. Not only is this typical of non-industrial cultures, I believe it represents the natural state of existence for Homo sapiens. Like all other animals, humans are healthy and robust when occupying their preferred ecological niche. Our niche happens to be a particularly broad one, ranging from near-complete carnivory to plant-rich omnivory. But it does not include large amounts of industrial foods.
In the next few posts, I'll discuss more specific data about the health of the Kitavans.
Wednesday, August 13, 2008
Is this guy for real? He is 52 years old?

So is this guy for real, he claims he has been doing Calorie Restriction since his 20s and is now 52 years old in that photo. I think one person Brian Delaney from the CR Society has run into him once before, so maybe this is real. We can clearly see from the animal experiments that the old CR monkeys look really young. Some CRers who are now approaching 40 look like they're in their 20's. So I wouldn't rule it out. It would be interesting to see Elixer in a video or something, rather than an image which can be photoshopped a bit.
There is a discussion over at Imminst about him. I don't know, you decide, do you think it's possible to look in 25-30 years old at 50? I think so, but have no idea if this guy is real because hes so mysterious lol.
Juvess no more?
As with the majority of skin creams I've run into a problem, yet again. I am thinking that i'll just have to go with the copper peptides to remodel the skin, and use just a general non oily moisturzer like oil of olay or something. The Juvess original contains somethings that could clog up pores and be comedogenic. For the majority of people the cream is fine but clearly not me. I will try an experiment and use it around the chin area and use an exfoliator like salicylic acid. The positives I noticed though were that in the morning my skin was much better, less red, better complexion, more soft and smooth. It's just approx 2 weeks after using it, it's like I'm 15 again. What I would give to have perfect skin! arghh! lol.
One thing I'm going to add back into skin care is Aloe Vera gel and apply at night, then wash off in the morning because I got told that direct exposure to sunlight will cause damage while using this.
One thing I'm going to add back into skin care is Aloe Vera gel and apply at night, then wash off in the morning because I got told that direct exposure to sunlight will cause damage while using this.
Tuesday, August 12, 2008
Letter to the Editor
I wrote a letter to the New York Times about their recent article "The Overflowing American Dinnerplate", which I reviewed here. The letter didn't get accepted, so I will publish it here:
In the article "The Overflowing American Dinner Plate", Bill Marsh cites USDA data showing a 59% increase in fat consumption from 1970 to 2006, coinciding with the doubling of the obesity rate in America. However, according to Centers for Disease Control NHANES nutrition survey data, total fat intake in the US has remained relatively constant since 1971, and has actually decreased as a percentage of calories. The apparent discrepancy disappears when we understand that the USDA data Marsh cites are not comprehensive. They do not include the fat contained in milk and meat, which have been steadily decreasing since 1970.
The change Marsh reported refers primarily to the increasing use of industrially processed vegetable oils such as soybean oil. These have gradually replaced animal fats in our diet over the last 30 years. Since overall fat intake has changed little since the 1970s, it cannot be blamed for rising obesity.
Monday, August 11, 2008
Quinoa Salad with Lime + Fresh Mint
 |
| Quinoa salad with fresh lime and mint. |
This is the post where I confess, Dear Reader, that I am now pear-shaped and lumpy and thick in the middle- obviously adept at gaining weight. I may even be considered gifted. This is not fun for me. But then, who promised fun during hip surgery recovery? Who said it would be easy? (Um, no one.) Throw menopausal hormone pandemonium into the sticky mix and you have a double roll nightmare.
I gained fifteen eighteen twenty damn pounds.
And who claimed that wedges of Green Chile Cornbread and Strawberry Chocolate Chip Scones and Peach Crisp were calorie-free, anyway? Certainly not moi. But geesh.
How much can a girl give up in one lifetime?
How much can a girl give up in one lifetime?
So the rumors are true. Your intrepid plucky gluten-free goddess is trying the South Beach Diet. Or as well as one can follow the famous low glycemic diet without the comfort of dairy foods (on my allergen verboten list). This should be interesting.
Or as well as one can follow the famous low glycemic diet without the comfort of dairy foods (on my allergen verboten list). This should be interesting.
Lucky for me I have a Guru.
Sunday, August 10, 2008
Rats on Junk Food
If diet composition causes hyperphagia, we should be able to see it in animals. I just came across a great study from the lab of Dr. Neil Stickland that explored this in rats. They took two groups of pregnant rats and fed them two different diets ad libitum, meaning the rats could eat as much as they wanted. Here's what the diets looked like:
The rest of the paper is interesting as well. Pups born to mothers who ate junk food while pregnant and lactating had a greater tendency to eat junk than pups born to mothers who ate rat chow during the same period. This underscores the idea that poor nutrition can set a child up for a lifetime of problems.
The animals were fed two types of diet throughout the study. They were fed either RM3 rodent chow alone ad libitum (SDS Ltd, Betchworth, Surrey, UK) or with a junk food diet, also known as cafeteria diet, which consisted of eight different types of palatable foods, purchased from a British supermarket. The palatable food included biscuits, marshmallows, cheese, jam doughnuts, chocolate chip muffins, butter flapjacks, potato crisps and caramel/chocolate bars.It's important to note that the junk food-fed rats had access to rat chow as well. Now here's where it gets interesting. Rats with access to junk food in addition to rat chow ate 56% more calories than the chow-only group! Here's what they had to say about it:
These results clearly show that pregnant rats, given ad libitum access to junk food, exhibited hyperphagia characterised by a marked preference for foods rich in fat, sucrose and salt at the expense of protein-rich foods, when compared with rats that only had access to rodent chow. Although the body mass of dams was comparable among all groups at the start of the experiment, the increased energy intake in the junk food group throughout gestation was accompanied by an increase in body mass at G20 [gestational day 20] with the junk food-fed dams being 13 % heavier than those fed chow alone.Hmm, this is remarkably reminiscent of what's happening to a certain group of humans in North America right now: give them access to food made mostly of refined grains, sugar, and industrially processed vegetable oil. They will prefer it to healthier food, to the point of overeating. The junk food then drives hyperphagia by interfering with the body's feedback loops that normally keep feeding behaviors and body fat within the optimal range. These data support the hypothesis that metabolic damage is the cause of, not the result of, "super-sized" food portions and other similar cultural phenomena.
The rest of the paper is interesting as well. Pups born to mothers who ate junk food while pregnant and lactating had a greater tendency to eat junk than pups born to mothers who ate rat chow during the same period. This underscores the idea that poor nutrition can set a child up for a lifetime of problems.
Subscribe to:
Posts (Atom)





